They Arrived on Crutches Expecting to Be Forgotten—But Behind the Barbed Wire of American Camps, Disabled German POWs Encountered a Secret World of Medical Care, Unsettling Kindness, and Quiet Acts of Dignity That Shattered Every Warning They Had Been Given, Forcing a Deep Psychological Reckoning About Defeat, Survival, and the Unexpected Humanity That Emerged While the War Still Raged Across a Burning World. VD
They Arrived on Crutches Expecting to Be Forgotten—But Behind the Barbed Wire of American Camps, Disabled German POWs Encountered a Secret World of Medical Care, Unsettling Kindness, and Quiet Acts of Dignity That Shattered Every Warning They Had Been Given, Forcing a Deep Psychological Reckoning About Defeat, Survival, and the Unexpected Humanity That Emerged While the War Still Raged Across a Burning World
When the transport ships crossed the Atlantic carrying wounded and disabled soldiers from Germany to the United States, many of the men onboard believed their fate had already been decided.
They had survived battlefields.
They had survived bombardments.
They had survived the chaos of surrender.
But they did not believe they would survive captivity—not in any meaningful sense.
For those who limped, who relied on crutches, who bore visible scars or permanent injuries, the fear was sharper. They expected to be seen not as prisoners of war protected by international standards, but as burdens. As liabilities. As men who had outlived their usefulness.
They had been told that the enemy would show no patience.
They had been warned that disability would invite neglect.
They braced for indifference.
What they encountered instead unsettled them far more deeply than cruelty might have.

Arrival: Fear Carried Ashore
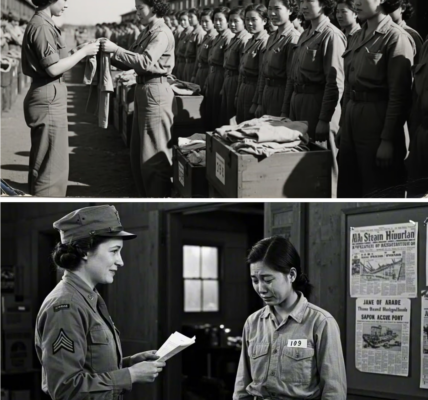
Many of the disabled prisoners had been captured during campaigns in North Africa and Western Europe before being transferred overseas. When they reached American ports, they were processed according to procedures influenced by the Geneva framework and monitored by neutral observers, including representatives of the International Committee of the Red Cross.
None of that reassured them.
Processing stations examined their medical conditions carefully. Names were recorded. Injuries documented. Prosthetics inspected.
The wounded expected rough handling.
Instead, they were directed toward medical units.
For some, it was the first structured treatment they had received in months.
That alone felt destabilizing.
Camps With Clinics, Not Abandonment
Several camps across the United States housed prisoners with medical needs. Facilities such as Camp Algona in Iowa and Camp Ruston in Louisiana maintained infirmaries staffed by American medical personnel trained to treat both domestic soldiers and foreign captives.
The existence of these clinics was not secret—but it was not widely publicized either.
Within the barbed wire perimeters stood modest medical buildings: examination rooms, recovery wards, supply closets stocked with bandages, antiseptics, and medications.
The disabled POWs had prepared themselves for the opposite.
They had expected to be left in drafty barracks.
They had expected minimal care.
Instead, they encountered intake assessments.
One former prisoner later recalled the shock of hearing an American doctor discuss the proper alignment of his damaged leg as if he were a regular patient.
“He spoke to me,” the man wrote years later, “not at me.”
That distinction lingered.
The Psychological Weight of Being Seen
In wartime, identity narrows quickly.
Uniform. Rank. Allegiance.
Injury complicates that identity.
A soldier who can no longer march or fire a weapon occupies a liminal space—no longer fully combatant, not yet civilian.
Many disabled German POWs arrived in America carrying not only physical wounds but internalized shame. They feared being viewed as failed soldiers.
Instead, medical staff treated injuries as clinical realities rather than moral verdicts.
Prosthetic fittings were adjusted.
Crutches were replaced when worn down.
Infections were monitored.
Some prisoners underwent corrective procedures to prevent long-term complications.
None of this erased captivity.
But it altered its emotional texture.
The men had expected punishment.
They encountered procedure.
They had expected dismissal.
They encountered documentation.
And in that administrative normalcy, something cracked open.
Suspicion Inside Compassion
The prisoners did not immediately trust what they experienced.
Kindness during conflict can appear strategic.
They wondered:
Was this for propaganda?
Was it a performance?
Were they being observed for hidden reasons?
The suspicion was not entirely irrational. War distorts motive.
Yet days turned into weeks.
Treatments continued.
Medications were dispensed consistently.
Physical therapy routines were established for those who required mobility rehabilitation.
Some camps organized structured exercise sessions for wounded men to prevent muscle atrophy.
The predictability itself was shocking.
Cruelty is chaotic.
Care is methodical.
They were encountering the latter.
Interactions With American Medical Staff
American doctors and nurses assigned to POW camps operated under military oversight. Their mandate included maintaining health standards for prisoners as required by international agreements.
But within those parameters, individual conduct varied.
In many cases, staff approached their work with professional detachment.
A fractured bone required stabilization.
A poorly healed wound required cleaning.
A fever required monitoring.
Political allegiance did not alter physiology.
One American nurse reportedly corrected a guard who addressed a disabled POW dismissively.
“He’s a patient first,” she said.
The prisoner did not understand every word—but he understood tone.
Dignity had been restored in a single sentence.
The Hidden Complexity for Guards
Compassion inside a prison camp was not universally celebrated.
Some American guards had lost friends or relatives overseas.
The sight of enemy soldiers receiving medical care stirred complicated emotions.
Yet regulations were clear.
The Geneva standards mandated humane treatment.
And oversight existed.
The presence of the International Committee of the Red Cross meant documentation could not be entirely ignored.
Over time, routine dulled sharp edges.
Guards witnessed the daily realities of injured men struggling to adjust to prosthetics or manage chronic pain.
Enemy became patient.
Patient became person.
The transition was subtle—but significant.
Rehabilitation and Work Adjustments
Disabled prisoners were often exempt from heavy labor details.
However, many expressed a desire to remain useful.
Camp administrators created light-duty roles:
Clerical assistance within the camp.
Library organization.
Workshop tasks involving carpentry or small repairs.
For some, purpose proved as healing as medicine.
One former artilleryman, who had lost partial mobility in one arm, began sketching architectural designs for small camp structures. American officers noticed his talent.
He was given access to drafting materials.
The act of being entrusted—even in limited capacity—challenged his expectation of being sidelined indefinitely.
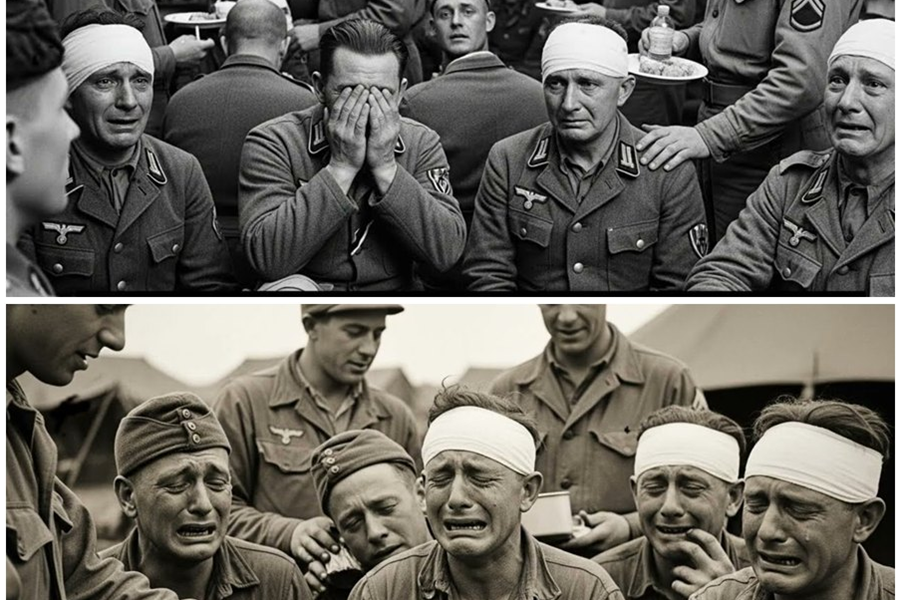
Emotional Aftershocks
Physical care addressed visible wounds.
But the deeper shock lay in psychological territory.
The men had been conditioned to expect contempt.
Instead, they encountered structured decency.
This did not produce instant gratitude.
It produced confusion.
One POW wrote in a monitored letter home:
“We were told that captivity here would strip us of everything. Yet they treat my leg as if it matters.”
The sentence was simple.
The implications were vast.
If the enemy valued his recovery, what else might be more complicated than he had believed?
Cultural Exchange in Unexpected Places
Inside infirmaries, conversations occasionally drifted beyond clinical necessity.
American staff asked about hometowns.
Prisoners asked cautious questions about American cities.
A nurse from the Midwest described winter harvest festivals.
A prisoner described river towns along the Rhine.
Shared geography humanized both sides.
No grand declarations occurred.
No ideological debates erupted.
Instead, fragments of ordinary life passed between individuals who months earlier might have faced one another across battle lines.
Resistance Within the Ranks
Not all prisoners welcomed this environment.
Some remained rigid in outlook, interpreting humane treatment as weakness.
A few discouraged fellow captives from expressing appreciation.
But prolonged exposure to consistent care made outright denial difficult.
Injuries improved.
Pain lessened.
Mobility increased.
The evidence was experiential.
Over time, even the most skeptical had to reconcile outcome with expectation.
Oversight and Documentation
American POW camps were subject to inspection.
Representatives of neutral organizations reviewed medical facilities, food standards, and living conditions.
Reports were filed.
Adjustments were recommended when necessary.
This oversight reinforced procedural care.
For disabled prisoners, it created a buffer against neglect.
The very existence of paperwork—charts, medical logs, supply inventories—served as proof that they had not been erased.
They existed in ink.
They existed in records.
They existed in a system that, while restrictive, acknowledged their physical condition as worthy of attention.
Letters That Changed Families’ Perceptions
Correspondence from disabled POWs sometimes carried unexpected tones.
Families back home, enduring scarcity and uncertainty, read descriptions of bandage changes and physiotherapy sessions with disbelief.
Some letters were cautious.
Others were quietly astonished.
The idea that American doctors were fitting prosthetics or correcting poorly healed fractures contradicted wartime caricatures.
For families, the information was destabilizing.
For the prisoners, writing it was transformative.
They were documenting a reality that forced introspection.
The Camp as a Psychological Crossroads
Captivity is never comfortable.
Freedom remained distant.
Uncertainty about the future lingered.
Yet within that constrained environment, the presence of medical care introduced a paradox.
They were confined—but treated.
Defeated—but not discarded.
The paradox demanded reflection.
If dignity could be extended in captivity, what defined strength?
If compassion could exist during active conflict, what defined enemy?
These questions did not resolve easily.
They settled into the background of daily routine, resurfacing in quiet hours.
Moments That Echoed
Several anecdotes from camp records and later recollections illustrate the subtle power of small acts:
-
An American orderly adjusting a prosthetic strap late at night so a prisoner could sleep without discomfort.
-
A camp physician explaining a surgical procedure in careful detail rather than issuing curt instructions.
-
A holiday card delivered to infirmary patients alongside standard rations.
None of these gestures altered geopolitical outcomes.
But they altered perception.
The War Beyond the Fence
While medical routines unfolded inside camps, the broader war continued.
News filtered in through approved channels.
Battles advanced.
Cities fell.
The knowledge that the conflict still burned elsewhere added complexity.
Why extend care when destruction continued abroad?
For the disabled POWs, the answer lay not in strategy—but in principle.
They were witnessing a system that separated medical ethics from battlefield rage.
That separation stunned them.
The Aftermath of Shock
As months passed, initial disbelief softened into cautious acceptance.
Some prisoners began assisting infirmary staff as translators or aides.
Others pursued educational courses offered within camps.
The psychological shock evolved into gradual adaptation.
The expectation of neglect had been replaced by lived experience of structured care.
This did not erase allegiance.
It did not rewrite history overnight.
But it complicated the narrative they carried.
Release and Memory
When the war eventually drew toward its end, questions of repatriation surfaced.
Disabled prisoners faced uncertainty about returning to a homeland transformed by conflict.
Yet many carried with them memories not of abandonment—but of unexpected dignity.
In postwar interviews decades later, some former POWs described American camp medical staff with a tone of sober respect.
They did not romanticize captivity.
But they acknowledged reality.
The fear they had carried across the ocean had not materialized in the form they anticipated.
A Quiet Reality Often Overlooked
Large-scale histories of global conflict focus on front lines and decisive battles.
Less frequently examined are the controlled environments where former enemies coexisted under regulation.
The experience of disabled German POWs in American camps reveals a layer of wartime history that resists simplification.
Within barbed wire boundaries, medical care functioned.
Within guard towers’ shadows, dignity appeared.
Within a system designed for containment, individual professionals chose adherence to ethical standards.
Redefining Defeat
Defeat often carries images of humiliation and erasure.
For these men, defeat became something more nuanced.
They were confined.
They were monitored.
They were not free.
Yet they were treated as patients when injured.
They were spoken to with professional respect.
They were given tools to recover mobility where possible.
The redefinition was quiet—but profound.
Survival Beyond the Physical
Survival is not solely the continuation of breath.
It is the preservation of self.
For disabled POWs expecting neglect, the discovery of medical attention and structured care forced a recalibration of identity.
They were not discarded.
They were not invisible.
In the midst of global conflict, they encountered a system that upheld standards even when emotions ran high.
That reality stunned them more than cruelty would have.
Because cruelty would have confirmed what they had been taught.
Compassion disrupted it.
And disruption, in wartime, can be the most shocking force of all.
Note: Some content was generated using AI tools (ChatGPT) and edited by the author for creativity and suitability for historical illustration purposes.