“Your Wound Is Bubbling…” — The Shocking 1944 Field Tent Decision That Saved an 18-Year-Old German Prisoner from a Near-Certain Death, As a British Surgeon Defied Convention, Carved Eight Inches into Rotting Muscle, Left the Leg Open to Air, and Changed the Future of Trauma Medicine in a Case That Haunted the War and Quietly Rewrote Surgical History Forever. VD
“Your Wound Is Bubbling…” — The Shocking 1944 Field Tent Decision That Saved an 18-Year-Old German Prisoner from a Near-Certain Death, As a British Surgeon Defied Convention, Carved Eight Inches into Rotting Muscle, Left the Leg Open to Air, and Changed the Future of Trauma Medicine in a Case That Haunted the War and Quietly Rewrote Surgical History Forever
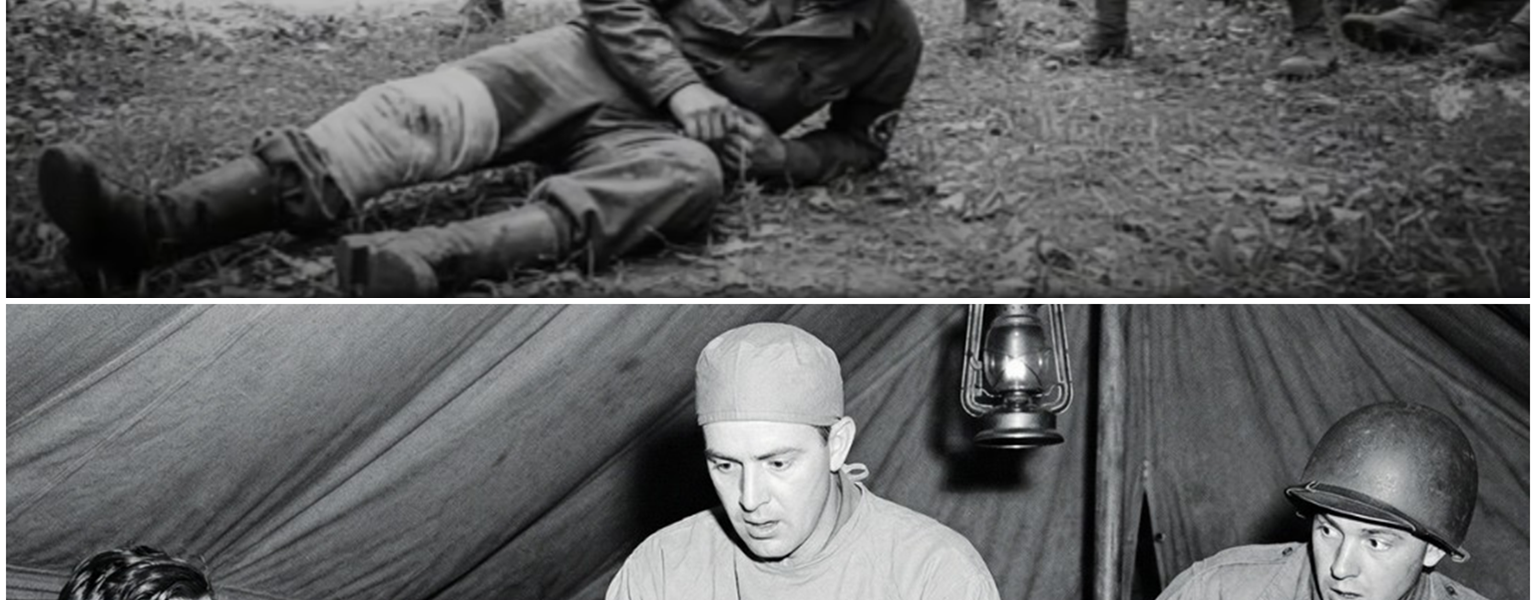
A Field Tent in France, August 1944
Late August 1944. Northern France.
Canvas walls snapped in a restless wind as stretcher-bearers moved in and out of a British field surgical unit positioned just behind advancing Allied lines. The war in Western Europe was shifting rapidly after the landings in Normandy. Transport columns jammed country roads. Casualties flowed in waves—Allied and Axis alike.
Inside one of those canvas tents lay an 18-year-old German prisoner of war named Franz.
He had been captured during a chaotic retreat. Three days earlier, amid confusion and exhaustion, he had fallen while moving with a transport column and struck his thigh against debris. The injury had torn the fabric of his uniform and cut deep into muscle. It bled, but not catastrophically. He wrapped it quickly and said nothing.
To report injury, in the chaos of retreat, could mean being left behind—or worse, accused of delaying movement.
So he walked.

For three days.
By the time British medical staff examined him, his thigh was swollen tight beneath the skin. The discoloration was unmistakable—patches of yellow-gray spreading into darkened red. When the surgeon gently pressed his gloved fingers against the wound, a faint crackling sensation could be felt beneath the surface.
And then there was the odor.
A sickly sweet smell that drifted into the tent before the dressing was fully removed.
The surgeon did not need long to understand.
Franz had developed gas gangrene.
What Gas Gangrene Meant in 1944


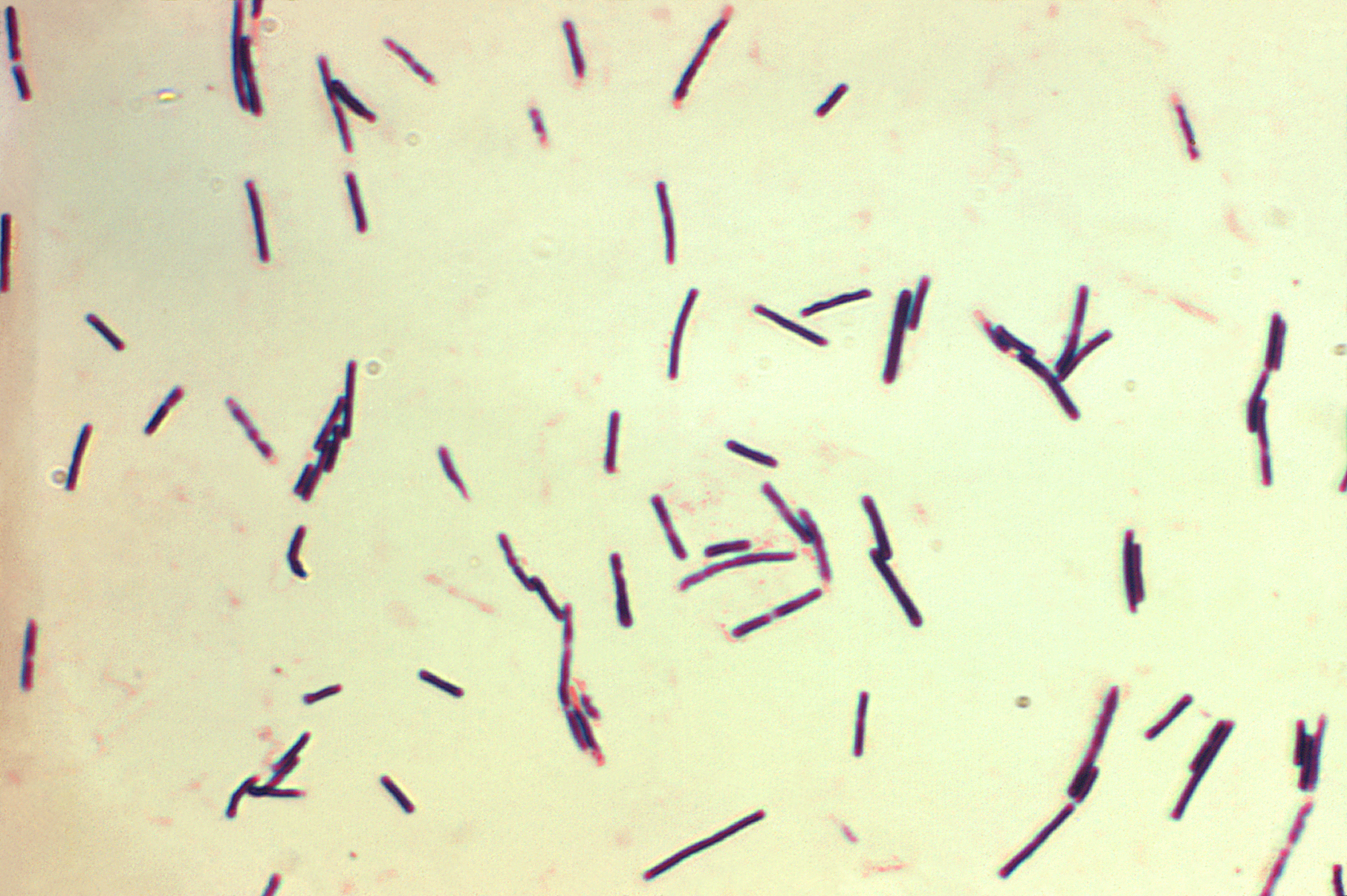
Gas gangrene—most commonly caused by Clostridium perfringens—was one of the most feared infections of wartime injuries.
The bacteria thrived in deep wounds with compromised blood supply. Once established, it produced toxins that destroyed muscle and connective tissue at alarming speed. Gas pockets formed as byproducts of bacterial metabolism, collecting beneath the skin and within muscle compartments. When pressed, they created a crackling sensation—crepitus—like crushed parchment.
Untreated, mortality rates exceeded 70 percent in many documented wartime cases.
In 1944, antibiotics such as penicillin were becoming more available but were still limited in supply. Surgical intervention remained the primary defense. And time was everything.
Based on the swelling and odor alone, the surgeon estimated Franz might have less than 36 hours before systemic toxicity overwhelmed him.
But there was another complication.
Franz was an enemy prisoner.
A Decision Under Strain
The British field hospital operated under international conventions requiring humane treatment of prisoners of war. Yet reality in late August 1944 was complicated. Resources were stretched. Surgical teams were overwhelmed. Supplies of antiseptic gauze, plasma, and anesthesia were rationed.
Some officers quietly questioned whether aggressive surgical measures should be used on German captives when Allied soldiers were arriving by the truckload.
The camp medical director was called.
The surgeon proposed a controversial option: radical debridement using what was known as the “open wound” technique.
This meant cutting deeply into infected tissue, removing every trace of compromised muscle, leaving the wound open to air rather than suturing it closed, and packing it with antiseptic dressings to prevent anaerobic bacteria from thriving.
It was aggressive. It was messy. It required time and supplies.
Some argued immediate amputation would be faster.
But the surgeon believed the infection had not yet destroyed the entire limb. If he could remove the dead tissue completely, Franz might survive—and keep his leg.
The director signed approval with a single line:
“Proceed, but document everything.”
Forty-Five Minutes That Changed a Life
Franz was placed on a wooden operating table under bright lamps powered by a generator outside the tent. Ether anesthesia was administered, though initial sedation was limited due to supply constraints.
For the first 15 minutes, Franz remained partially conscious. He was given a wooden dowel to bite down on.
Witnesses later wrote that he bit so hard the dowel splintered.
The surgeon began by enlarging the wound. What had once been a jagged tear became an incision nearly eight inches long. Layers of muscle were exposed.
Healthy muscle bleeds and contracts when cut. Infected muscle does not. It appears gray, sometimes greenish, and soft. It does not respond.
The surgeon removed tissue layer by layer, cutting until he reached viable, bleeding muscle.
Assistants sponged continuously. The odor intensified as deeper pockets were opened. Gas bubbles rose and escaped audibly.
The femur became visible at the base of the wound in certain areas.
When the surgeon finally stopped, the cavity measured roughly eight inches long and four inches wide, deep enough to see structures that would never normally be exposed outside a surgical theater.
But the tissue that remained was alive.
The wound was not closed.
Instead, it was packed tightly with antiseptic gauze and left open.
Why Leave a Wound Open?
Modern readers might find it counterintuitive that a wound would be left open intentionally. But in 1944, surgeons were learning—often through brutal necessity—that closing contaminated wounds could trap bacteria inside, creating the perfect environment for further infection.
The “open wound” technique allowed oxygen to penetrate. Clostridium perfringens thrives in low-oxygen environments. Exposure slowed its growth.
By removing every trace of necrotic tissue and leaving the area open, surgeons aimed to give the body a fighting chance.
Later post-war analyses would show that radical debridement combined with staged closure improved survival rates by approximately 15–20 percent compared to immediate amputation in certain early-detected cases.
Franz became one of those statistics.
Three Months of Uncertainty
Franz was transferred to a larger Allied medical facility in Belgium for ongoing care.
The wound required daily inspection. Dead tissue sometimes reappeared at the margins and had to be removed. Gauze packing was changed carefully to avoid damaging newly forming granulation tissue.
The pain was substantial. Infection control required vigilance. Nutrition was increased to support healing.
Weeks passed.
The wound gradually began to fill in from the bottom up—a process known as healing by secondary intention.
Only after the infection was fully resolved did surgeons begin staged closure procedures, gradually reducing the wound size and reconstructing tissue coverage.
Franz would undergo multiple smaller operations across three months.
By late autumn, he could stand with assistance.
A Permanent Limp—and a Preserved Limb
Franz never regained full strength in his thigh. Muscle mass lost to infection and removal could not be restored entirely.
He walked with a permanent limp.
But he walked.
He kept his leg.
In later years, according to family accounts, Franz told his children, “The leg was a gift.”
It was not a statement of nationalism or allegiance. It was a statement about survival—and about a surgeon who chose time-consuming intervention over expediency.
Franz lived until 1997.
He was 71 years old.
The Broader Medical Impact


Cases like Franz’s did not remain isolated anecdotes.
The directive to “document everything” ensured that operative notes, wound measurements, infection progression, and outcomes were recorded meticulously.
After the war, these records were analyzed alongside hundreds of similar cases from Allied and Axis medical units.
Patterns emerged:
-
Early radical debridement significantly improved survival.
-
Leaving contaminated wounds open reduced recurrence of anaerobic infection.
-
Staged closure after infection control preserved more limbs than previously believed possible.
-
Immediate amputation was not always the superior choice.
These findings influenced trauma protocols in subsequent conflicts, including the Korean and Vietnam wars, where rapid evacuation and early aggressive surgical management became standard practice.
Civilian trauma care also evolved. Techniques pioneered under wartime necessity became foundational principles in emergency surgery.
Today, surgical residents are taught the importance of debridement, staged reconstruction, and infection control protocols that trace lineage directly to lessons learned in 1944.
Ethics in a Canvas Tent
Franz’s case also illuminates an ethical dimension often overshadowed by battlefield narratives.
Treating an enemy prisoner with the same aggressive care as one’s own soldiers was not universally embraced in strained wartime environments.
Yet the decision to proceed reflected adherence to medical ethics that transcend nationality.
The field surgeon later wrote in a private letter:
“A wound does not carry a flag.”
In that tent, the bacteria did not distinguish between uniforms. Nor did the surgical principles required to stop them.
The Science Behind the Survival
Gas gangrene progresses with frightening speed because toxins produced by the bacteria damage blood vessels, limiting oxygen supply and accelerating tissue death.
Radical debridement interrupts that cascade by physically removing toxin-producing colonies and restoring oxygen exposure to remaining tissue.
In Franz’s case, the infection had not yet reached systemic circulation in lethal concentration.
Timing was everything.
Had he waited another day to seek treatment, the outcome might have been different.
From Battlefield to Textbook
In post-war surgical conferences, cases like Franz’s were presented as evidence supporting a shift in doctrine.
Rather than defaulting to amputation in severe limb infections, surgeons increasingly advocated for:
-
Early detection
-
Aggressive but targeted tissue removal
-
Open wound management
-
Delayed closure after infection control
These principles became embedded in trauma surgery training programs worldwide.
Modern disaster response, industrial accident care, and even complex orthopedic procedures owe part of their evolution to those wartime innovations.
A Quiet Legacy
Franz never became famous. He did not publish memoirs. He did not seek recognition.
He built a life after the war. Worked. Raised children. Walked with a limp that reminded him daily of a tent in France and a surgeon who chose to fight for his leg.
His medical file, preserved in archives, became one of many data points shaping surgical doctrine.
But behind the clinical terminology—debridement, secondary intention, staged closure—was an 18-year-old who once lay on a wooden table with his future measured in hours.
The Line That Saved a Life
“Proceed, but document everything.”
It was a simple instruction.
Yet it encapsulated two essential forces: action and knowledge.
Action saved Franz in the moment.
Documentation ensured that his case would save others.
Thousands of lives in later conflicts and civilian emergencies were influenced by the cumulative understanding built from such decisions.
When Medicine Transcends the Battlefield
War accelerates destruction.
But it also accelerates learning.
The same conditions that create devastating injuries can, paradoxically, advance medical science when physicians refuse to compromise standards.
Franz’s story is not about heroism in combat.
It is about a choice made in a canvas tent under pressure.
A choice to cut deeper rather than cut off.
A choice to invest time in a life that some might have considered expendable.
A choice that echoed through decades of surgical education.
The Gift of a Scar
The scar Franz carried was extensive—eight inches long at its widest point, textured from multiple closures.
He reportedly rarely covered it at home. When asked about it, he did not speak of enemies or blame.
He spoke of a doctor who “would not let the leg go.”
In the end, the wound that once bubbled with infection became something else entirely—a marker of survival, of medical evolution, and of a moment when ethics and skill converged under canvas.
The war moved on. Armies advanced. Borders shifted.
But inside that field tent in August 1944, a surgical decision quietly reshaped the future of trauma care.
And an 18-year-old who might have become another statistic instead walked into a long life—limping, yes—but walking all the same.
Note: Some content was generated using AI tools (ChatGPT) and edited by the author for creativity and suitability for historical illustration purposes.



